COVID-19
Argentine scientists developed a device that allows two patients to safely use one ventilator
It could increase the capacity of intensive care to be required before temporal lack of equipment because it can be used indefinitely

{kind=link}
A team led by Guillermo Artana, CONICET principal researcher at the Facultad de Ingeniería of the Universidad de Buenos Aires, designed a biosafety device that enables the use of one ventilator for two patients –dual ventilation–.
The idea came up in March, when the researchers sought to enhance the dual ventilation that was being implemented as emergency resource in several countries affected by the overload of the health system. In those cases, there was no device thought and designed for this purpose, which lost the capabilities of the team and there was risk that one patient would contaminate the other with pathogens.
“We thought it was important to try to enlarge the capabilities of the breathing machines in stock and of those that will be produce so as to provide a rapid response; the situation that we are proposing is in the case of an overflow.”
“This option provides the State with certain flexibility to manage rationally the stock of breathing machines. The production is not very sophisticated, it requires to be assembled in a clean environment with hygienic conditions. This could be quickly in hospitals,” says Artana.
The device was designed considering that it should be universal and that it can be used in any type of equipment regardless of the model. The researchers used the guidelines provided by the FDA (Food and Drugs Administration) in April in the United States. “In addition, it complies with the standards set by SATI (Sociedad Argentina de Terapia Intensiva), which explains the minimum requirements for a device that ventilates in an emergency condition such as the current one,” the scientist adds.
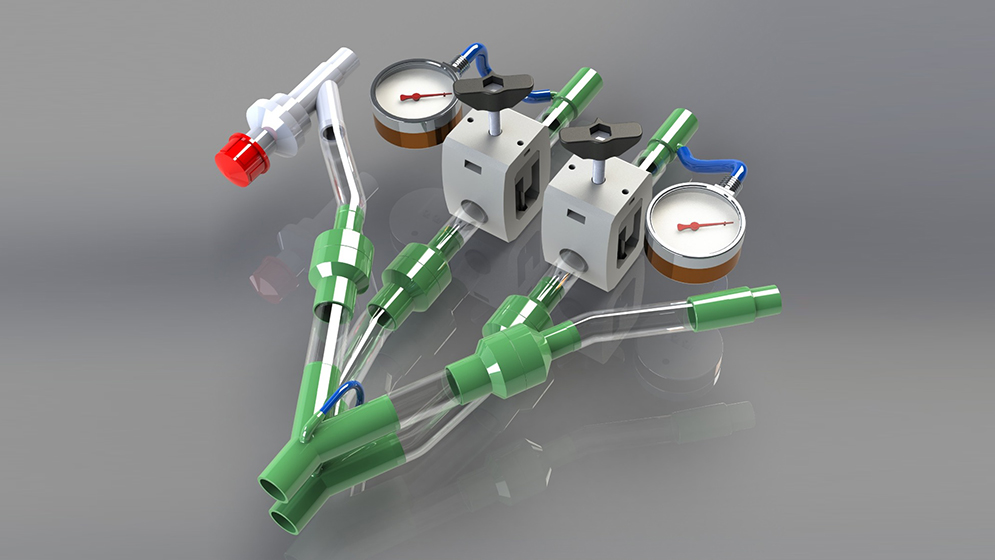
The development has three valves that regulate what is known as peak and residual pressure. On the one hand, it has two valves that are in charge of regulating the peak pressure (they cause a drop in the pressure between what the breathing machine marks and what reaches the person). On the other hand, it has a third valve known as ‘threshold’ or ‘PEEP’, which acts on the residual pressures: one of the patients receives the value that is set in the ventilator and the other, with the special valve, a modified value.
“In addition, doctors observe with manometers [devices that measure pressure] what pressure reaches the patient to which it is added what is sensed by the respirator. This incorporates a learning curve for doctors, who can be trained in just some hours and become familiar with the equipment,” the researcher adds.
The study was conducted mainly at the Laboratorio de Fluidomecánica of the Facultad de Ingeniería of the UBA and it was initially supported by UBATEC S.A. Besides, the study comprised the participation of: Cátedra de Anestesiología of the Facultad de Ciencias Veterinarias of the same university, and the hospital de Clínicas for some validations. Other institutions that collaborated with important numerical simulations were the simulation centers of YTEC (YPF-CONICET) and of CIMEC, (CONICET- Universidad Nacional del Litoral). “A large group of people have worked in this study. We are very pleased to see it in its final stage. This study was supported by a lot of people,” Artana states.